with complete block of renal blood flow (zero GFR) it takes several days for creatine in plasma to double.
Creatinine can increase in multiple ways independent of GFR; e.g., blocked secretion of Cr by tubule cells
BUN can also increase independent of kidney problems; e.g., GI bleed (BUN level increases in upper GI bleeding because patients become prerenal, secondary to blood loss)
AKI
- fluid overload
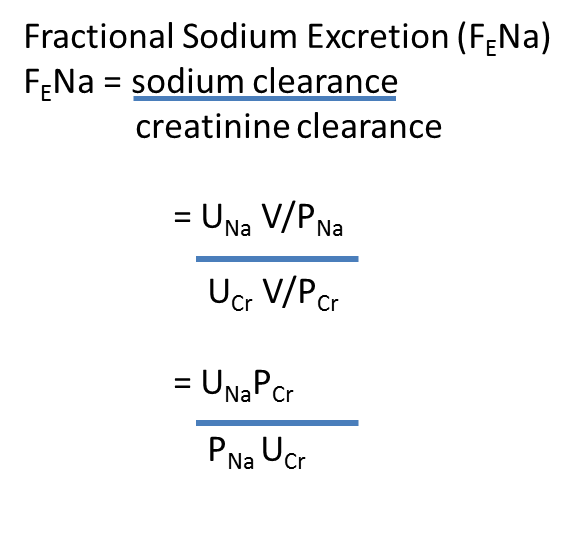
Fractional excretion of sodium (FeNa) = sodium clearance/creatinine clearance
= UNaV/PNa
AKI
1. pre-renal -
- decreased fractional excretion of sodium (stimulation of aldosterone) (unless patient is on diuretics)
- BUN/Cr > 20 hypovolemia stimulates ADH which increases urea reabsorption in medulla = increased BUN.
- fractional excretion of urea < 35% (low) (reliable measure for patient on diuretics where FeNa is higher due to diuretic)
- decreased GFR due to low blood pressure/hypoperfusion. compensated by autoregulation of GFR; i.e., afferent arteriole vasodilation mediated by prostaglandins (blocked by NSAIDS). also compensated by efferent arteriole vasoconstriction mediated by AT 2 (blocked by ACE inhibitors and ARB).
- IV contrast dyes can vasoconstrict afferent arterioles
- tubular necrosis (ATN) - ischemic; e.g., following prolonged pre-renal hypoperfusion or toxic
endothelial damage - tubular injury = inflammation, obstruction of tubule
dilute urine, FeNa increased, FeUrea increased
oligouria - reduced urine volume: normal glomeruli but damged tubules - mechanisms =
- blockage of lumen by dead cells, blocked urine enters blood ("back leak");
- increased tubuloglomerular feedback Na Cl to MD signals afferent arteriole vasoconstriction
indication for dialysis = no response to diuretics, also hyperK, metabolic acidosis refractory to treatment; uremia; progressive azotemia (BUN > 80-100 mg.dL)
- interstitial (AIN)
lymphocytes and eosinophils in interstital space
normal urine output (tubules not blocked)
- glomerular (Ann Richards) (AGN) acanthocytes (Mickey Mouse hat)
- vascular - microvascular (TTP), macrovascular (renal artery thrombosis)
increased pressure in Bowman's capsule decreases GFR. hydronephrosis = dilation of kidney
BUN level increases in upper GI bleeding not necessarily because patients become prerenal secondary to blood loss, but because protein in blood is broken down into urea in the GI tract and this is absorbed to blood.
ReplyDeleteBUN level cannot only increase in upper GI bleeding because patients become prerenal secondary to blood loss but because protein in the blood is broken down into urea and the urea is reabsorbed into the blood
ReplyDelete